
Ultrasound-Guided trigger Finger (Tendovaginitis Stenosans) Surgery
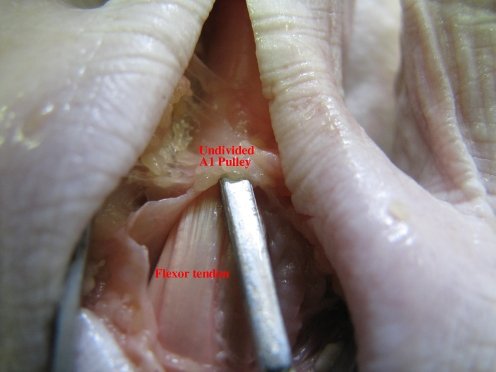
The tendons on the palm side bend the fingers. These are known as the flexor tendons. On the fingers and on the thumb there are small rings, through which the flexor tendons run. The collective of these flexor tendons and their tunnel-like structure rings is called the pulley system. The trigger finger syndrome takes place within this structure.
Flexor pulley system consists of following:
– Palmar Aponeurosis pulley
– Annular pulleys
– Cruciform pulleys.
Together, these form a fibro-osseous tunnel on the palmar aspect of the hand through which passes the deep and superficial flexor tendons.
Flexor tendon pulley system maintains flexor tendons close to joint’s axis of motion and there is one of them on each finger.
If these tunnel-like structures become too narrow, the flexor tendons are unable to glide along freely inside them. This results in extremely painful and irritating blocking which is reversed in a jerking manner with effort (snapping or triggering of the finger). Often, patients report that the snapping follows an unusual strenuous activity (such as gardening, carrying for long periods of time). During these – often unfamiliar – activities, pressure is exerted on the flexor tendons of the fingers and the tendon sheaths become thicker obstructing the gliding motion of the flexon tendon.
This condition can be alleviated by the administration of orticosteroid injections. These are shots with a needle into a joint (such as the finger) or a tendon. Corticosteroids work by reducing the inflammation of the finger. The injection itself might also help to relieve the pressure on the tendon. While these injections resolve the inflamation and ease the gliding of tendons through it’s sheaths, this is only a temporary solutions and injectios will haVe to be re-adminitered to maintain good function of the joint.
The only proven way this condition can be permanently resolved has been through surgery. Blind percutaneous A1 pulley release was first described by Lorthior in 1958 (Paulius and Maguina, 2009). This operation can be done without any special preparation and can obtain the effect equal to that of an open procedure.
Besides, this procedure has many advantages, including shorter recovery time, avoidance of scar tenderness, and application in the outpatient setting (Rajeswaran et al., 2009; Rojo-Manaute et al., 2010, 2012a,b; Smith et al., 2010). However, there is still a potential risk of damage to the tendon and neurovascular structures. Also, it is difficult to confirm whether the release is complete or not during operation because of invisualization directly (Lee et al., 2018).
There are studies about ultrasonography-guided percutaneous A1 pulley release with the needle knife showing that the ultrasonography-guided surgery has significantly better grade
postoperatively and reached to 100% complete release in one time compared to the blind group. Moreover, no complications had been recorded in the ultrasonography-guided group.
Ultrasound provides a direct and precise visualization of the thickness, width and location of A1 pulley lesion. The combined use of ultrasound and the needle knife can achieve the best result for trigger finger ( tendovaginitis stenosans). Moreover, the combination changes the traditional opinion and operator-dependent mode that were once widely adopted in hospitals in chinese medicine.
US scans performed with high-resolution, broad-band high frequency transducers allows superb visualization of the flexor tendons of the hand and the annular digital. Both the color doppler mini linear WiFi ultrasound scaner SIFULTRAS-3.51 and the Mini Linear Handheld WiFi Ultrasound Scanner SIFULTRAS-3.5 Comes with needle guide holder. Hence it can be directly set to the guide pin frame. Coupled with the software that can quickly locate the depth and diameter of puncture’s navigation.
The standard approach therefore is an in-plane technique where there is visualisation of the long axis of the needle knife and the needle tip is better tracked.
This procedure is performed by: Orthopedic hand surgeons.


[launchpad_feedback]